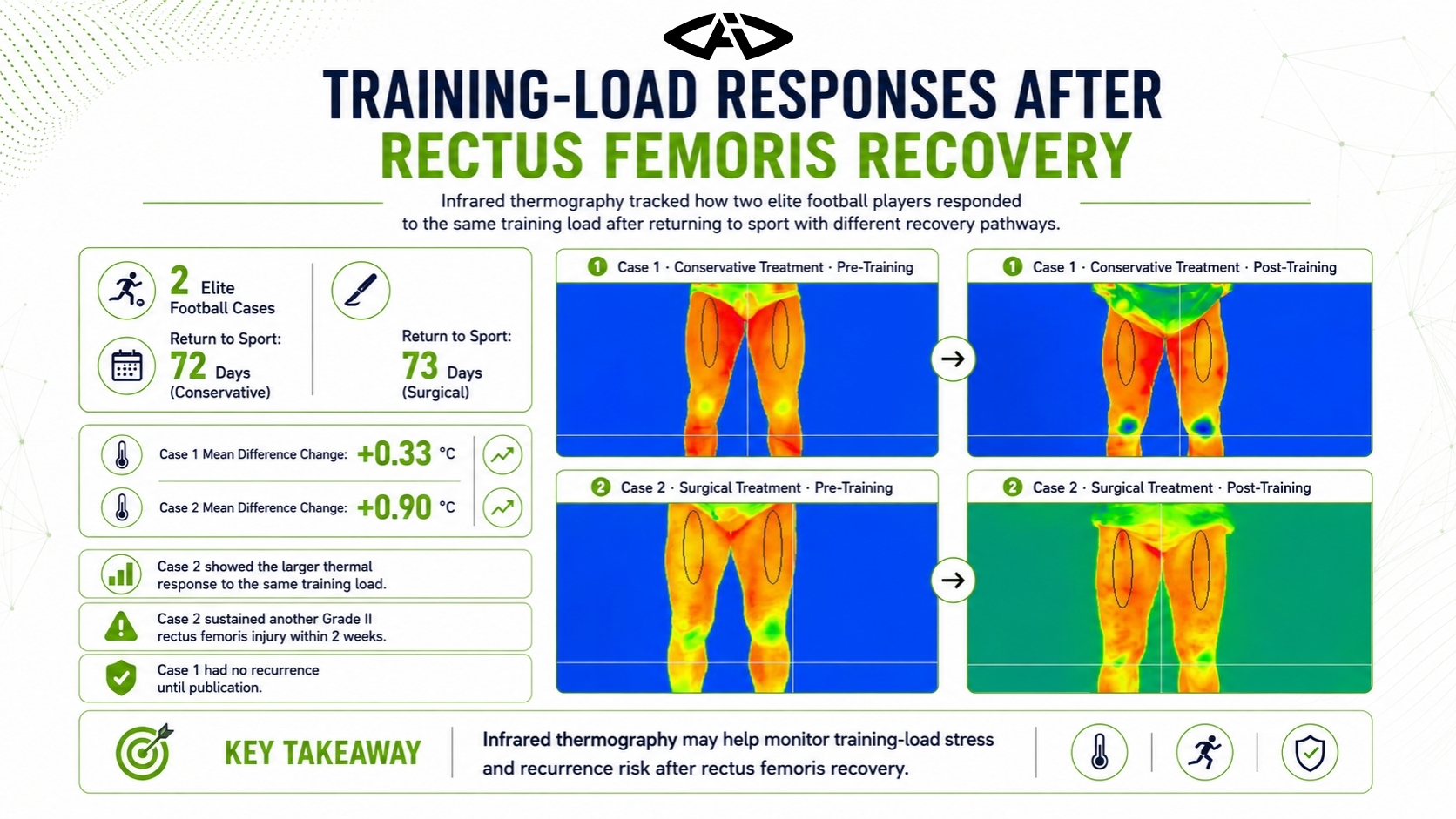
Two elite football players who returned to sport after conservative and surgical treatment were compared under the same training load using infrared thermography. The surgically treated player showed a larger side-to-side thermal change and sustained another injury in the same region two weeks later.
Study Objective
The rectus femoris plays an important role in football actions such as shooting, fast running and coordinated hip-knee movement. Proximal rectus femoris tears are rare, and there is no standard consensus on how athletes should be followed after conservative or surgical treatment.
This study compared the thermal responses of two football players who returned to sport after different treatment pathways and completed the same training programme.
Key message: Thermal response to the same training load after return to sport may provide additional information about adaptation and possible recurrence risk.
Case Profiles
Two elite football players with Grade III proximal rectus femoris injuries were evaluated.
| Case | Age | Injury region | Treatment | Return to sport |
|---|---|---|---|---|
| Case 1 | 22 | Left proximal rectus femoris | Conservative | 72 days |
| Case 2 | 31 | Right proximal rectus femoris | Surgical | 73 days |
Both athletes returned to training after rehabilitation and underwent thermal imaging before and after the same training load.
Case 1: After Conservative Treatment
Before training, the mean temperature difference between the right and left rectus femoris regions was 0.40 °C. After training, it increased to 0.73 °C.
| Measurement | Before training | After training | Change |
|---|---|---|---|
| Mean difference | 0.40 °C | 0.73 °C | +0.33 °C |
| Minimum difference | 0.57 °C | 1.02 °C | +0.45 °C |
| Maximum difference | −0.11 °C | −0.29 °C | 0.18 °C |
Although the thermal difference increased after training, Case 1 had no recurrence up to the publication of the study.
Case 2: After Surgical Treatment
Before training, the mean temperature difference was −0.69 °C. After training, it changed to 0.21 °C.
| Measurement | Before training | After training | Change |
|---|---|---|---|
| Mean difference | −0.69 °C | 0.21 °C | +0.90 °C |
| Minimum difference | −0.70 °C | −0.19 °C | +0.51 °C |
| Maximum difference | −0.30 °C | 0.75 °C | +1.05 °C |
Case 2, who returned after surgical treatment, showed a larger thermal response to the same training load than Case 1.
Comparing the Two Cases
Despite completing the same training programme, the two players showed clearly different thermal responses.
- Case 1 showed a +0.33 °C change in mean temperature difference.
- Case 2 showed a +0.90 °C change in mean temperature difference.
- Case 2 showed a +1.05 °C change in maximum difference.
The study reported that the athlete who recovered through surgery displayed a greater thermal response to training stress.
Important finding: Case 2 sustained a Grade II rectus femoris injury in the same region two weeks after the thermal assessment.
Interpretation
The authors stated that Case 1 appeared to adapt better to the stress caused by training, while Case 2 showed a greater thermal change.
The findings suggest that thermal imaging may support:
- assessment of training-load effects in athletes with injury history,
- monitoring of side-to-side temperature changes,
- recognition of early signals related to recurrence risk.
Roles of MRI and Thermography
The paper identified MRI as the gold standard for structural injury diagnosis. However, MRI and ultrasound do not directly show how the athlete responds physiologically to a specific training load in real time.
Thermography made it possible to compare pre- and post-training thermal changes and visualise the athlete’s response to load.
Limitations
The study included only two cases. It therefore cannot establish that one treatment method is generally superior to the other.
Although the authors suggested that conservative treatment may be associated with better adaptation in these cases, larger studies are required.
Conclusion
Two elite football players who returned after different treatments showed different thermal responses to the same training load. The larger change observed in the surgically treated player, followed by another injury in the same region two weeks later, highlighted the potential value of thermography in follow-up.
Infrared thermography may serve as a supportive method for monitoring training stress and possible recurrence signals after rectus femoris recovery.


